Apical & Subcostal View
Angela Mordecai, DNP, CRNA and Bailey Freeman, DNP, CRNA
Quick Facts
- Apical views offer the best alignment for all four chambers
- Subcostal views are often obtainable when other views fail
- IVC view provides valuable information about volume status
- These views are essential for comprehensive cardiac assessment
Indications
Apical and Subcostal views in cardiac POCUS are indicated for:
- Comprehensive evaluation of all cardiac chambers
- Focused right heart assessment
- Volume status assessment
- Alternative windows when parasternal views are limited
Relative Contraindications
- Apical view may be difficult in obese patients
- Limited by hyperinflated lungs (COPD, asthma)
- Recent abdominal surgery (for subcostal views)
Procedure
Equipment Needed:
- Cardiac (phased array) probe
- Ultrasound gel
- Patient positioning specific for each view
- Ultrasound machine with cardiac preset
View-Specific Techniques
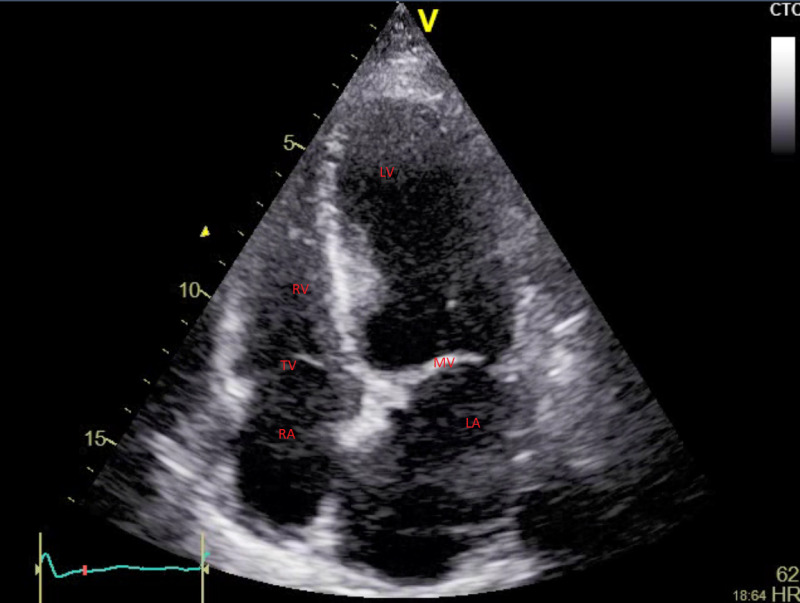
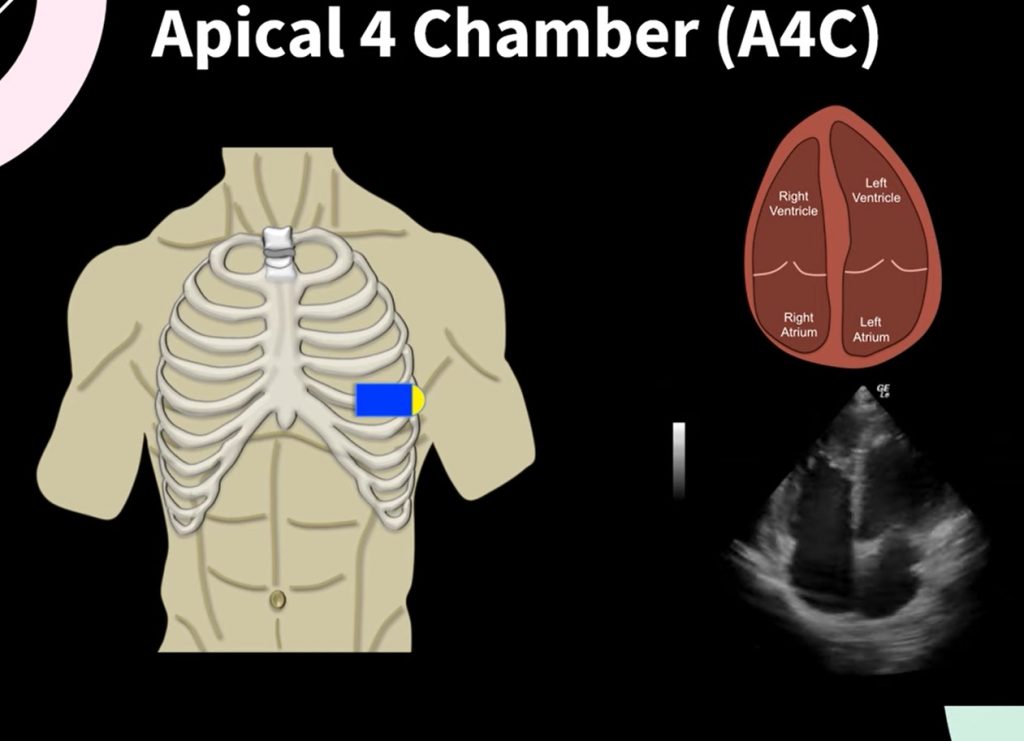
APICAL FOUR-CHAMBER VIEW
- Position patient in left lateral decubitus position
- Palpate the point of maximal impulse (PMI)
- Place probe at the PMI
- Direct indicator toward left axilla or 3 o’clock position
- Angle probe slightly medially and superiorly
- Adjust depth to visualize all four chambers
- Ensure interventricular septum appears vertical
SUBCOSTAL VIEW
- Position patient supine with knees slightly flexed
- Place probe just below xiphoid process
- Direct indicator toward patient’s right side (3 o’clock)
- Apply firm pressure angling toward left shoulder
- Flatten probe against abdomen
- Have patient take deep breath to bring heart closer to probe
- Adjust depth to visualize all four chambers
IVC VIEW
- From subcostal four-chamber position, rotate probe toward patient’s right
- Direct indicator toward patient’s head
- Identify IVC entering right atrium
- Adjust to longitudinal axis of IVC
- Follow IVC distally for approximately 2-3 cm
- Observe respiratory variation during quiet breathing
View-Specific Details
APICAL FOUR-CHAMBER
Anatomy Visualized
- Structures seen:
- All four cardiac chambers
- Interventricular septum
- Interatrial septum
- Mitral valve
- Tricuspid valve
- Normal relationships:
- LV apex at bottom of screen
- Atria at top of screen
- RV to the right of screen
- LV to the left of screen
- RV approximately 2/3 the size of LV
Clinical Assessment
- Function evaluation:
- Global LV and RV function
- Regional wall motion
- Septal motion
- Valve motion
- Structural assessment:
- Chamber size comparison
- Septal integrity
- Valve morphology
- Pericardial space
SUBCOSTAL FOUR-CHAMBER
Anatomy Visualized
- Structures seen:
- All four cardiac chambers
- Interventricular septum
- Interatrial septum
- Pericardium (excellent view)
- Portion of liver (anterior to heart)
- Normal appearance:
- Heart viewed from inferior aspect
- RV appears anterior
- RV approximately 2/3 the size of LV
- Thin pericardium without effusion
Clinical Assessment
- Function evaluation:
- Global cardiac function
- Alternative window when others limited
- First choice in cardiac arrest
- Structural assessment:
- Excellent for pericardial effusion
- Good for RV size and function
- Septal motion and position
IVC VIEW
Anatomy Visualized
- Structures seen:
- Inferior vena cava
- Right atrium junction
- Hepatic veins (often visible)
- Liver tissue surrounding IVC
- Normal appearance:
- Tubular structure entering RA
- Diameter 1.5-2.1 cm
- Collapses >50% with inspiration (in spontaneous breathing)
Clinical Assessment
- Volume status evaluation:
- Diameter measurement 2-3 cm from RA junction
- Respiratory variation assessment
- Correlation with clinical status
- Right atrial pressure estimation:
- IVC 50% collapse: normal RA pressure (0-5 mmHg)
- IVC >2.1 cm with 15 mmHg)
- Intermediate findings suggest moderate elevation (5-15 mmHg)
Confirmation Steps
APICAL FOUR-CHAMBER CONFIRMATION
- Verify key structures:
- All four chambers visualized
- Interventricular septum appears vertical
- Apex visible at bottom of screen
- Chamber identification:
- LV left side, apex at bottom
- RV right side, approximately 2/3 size of LV
- LA left top, approximately equal to RA
- RA right top
- True apical view confirmed by:
- LV apex visible and centered
- All four chambers approximately equal depth
- Interventricular septum vertical, not angled
SUBCOSTAL CONFIRMATION
- Verify four chambers:
- RV anterior (top of screen)
- LV posterior
- RA right side
- LA left side
- Pericardium visualization:
- Thin echogenic line surrounding heart
- No effusion present
- Liver visualization:
- Homogeneous tissue anterior to heart
- Used as acoustic window
IVC CONFIRMATION
- Verify true longitudinal view:
- IVC appears as tubular structure
- RA junction visible
- Hepatic vein junction often visible
- Proper measurement:
- Measure 2-3 cm from RA junction
- Perpendicular to vessel long axis
- Assessment during quiet breathing
- Respiratory variation:
- Observe diameter changes during respiration
- Note percentage of collapse with inspiration
Documentation Requirements
- Still images of each view
- For IVC: Measure maximum diameter and respiratory variation
- Document abnormalities in chamber size or function
- Video clips showing dynamic function
- Estimated right atrial pressure based on IVC
SCOPE GUIDE
Strategies & Clinical Optimization
Patient Positioning Optimization
- Apical view:
- Extreme left lateral position for difficult windows
- Left arm raised above head
- Consider slight reverse Trendelenburg
- Subcostal view:
- Knee flexion to relax abdominal muscles
- Deep inspiration to bring heart closer to diaphragm
- Consider slight Trendelenburg in difficult cases
- IVC view:
- Supine position optimal
- Avoid Valsalva maneuver during assessment
- Observe during normal quiet breathing
Technical Optimization Tips
- Apical challenges:
- Careful PMI palpation before probe placement
- Try multiple locations around apex area
- Use respiratory variation to advantage
- Subcostal challenges:
- Increase pressure gradually to displace bowel gas
- Try slightly right or left of midline
- Patient-assisted breathing techniques
- IVC assessment:
- Measure 2-3cm from RA junction
- Assess respiratory variation during normal breathing
- Verify true longitudinal plane
Probe Handling Techniques
- Apical view:
- Slower, more deliberate probe movements
- Small adjustments in angulation
- Patience to find optimal window
- Subcostal view:
- Use more firm pressure
- Flatten probe against abdomen
- Coordinate with patient breathing
- IVC assessment:
- Rock probe to ensure true long axis
- Maintain stable position during respiratory cycle
- Follow vessel from RA junction distally
Pearls
- RV should be no larger than 2/3 the size of LV in apical view
- IVC >2.1cm with <50% collapse suggests elevated RA pressure
- Subcostal view is often your best option in cardiac arrest situations
- For apical view, palpate PMI before probe placement
- Use slower, more deliberate probe movements for fine adjustments
View-Specific Tips
- Apical challenges:
- Difficult in COPD – try more lateral approach
- Look for “true apex” with LV tapered appearance
- Avoid foreshortening by identifying true apex
- Subcostal strengths:
- Often available when other views fail
- Excellent for pericardial effusion assessment
- First choice in trauma or arrest
- IVC interpretation:
- Changes in mechanical ventilation (opposite collapse pattern)
- Integration with clinical context essential
- Serial measurements often more valuable than single assessment
Quick Resources
IVC Interpretation
(diagram)
Key Measurements
- Normal IVC diameter: 1.5-2.1 cm
- Normal IVC respiratory variation: >50% collapse
- Normal RV:LV ratio: ≤0.6
- Normal RA pressure: 0-5 mmHg
Key Images/Diagrams
Anatomical Views
- Apical four-chamber orientation
- Subcostal four-chamber orientation
- IVC measurement location
- Chamber identification guide
Clinical Interpretation
- IVC diameter interpretation chart
- Normal chamber size relationships diagram
- RA pressure estimation guide
- Respiratory variation assessment
Reference Materials
- Normal vs. abnormal apical view images
- Pericardial effusion examples
- IVC respiratory variation examples
- Probe positioning illustrations
References
1. International consensus guidelines on IVC assessment
2. American Society of Echocardiography guidelines for chamber quantification
3. American College of Emergency Physicians. ACEP Policy Statement: Emergency Ultrasound Imaging Criteria Compendium
Media Attributions
- Apical 4-Chamber is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- Subcostal is licensed under a CC BY-NC (Attribution NonCommercial) license
- Apical 4 Chamber © Matthew Lipton, MD is licensed under a CC BY (Attribution) license
