Bronchospasm
Kristin Barkley, DNP, CRNA
Quick Facts
- Bronchospasm is an acute episode of increased airway resistance that can occur at any time from induction to PACU.
- Caused by sudden constriction of smooth muscle in the bronchioles.
- More common in patients with:
- History of asthma, COPD, or chronic bronchitis
- Recent upper respiratory infection (within 2 weeks)
- Potential complications: hypoxia, hypercapnia, V/Q mismatch, and cardiopulmonary compromise.
- Anesthetic-related factors:
- Light plane of anesthesia
- Airway instrumentation (e.g., intubation with ETT)
- Irritants such as aspiration contents, secretions, volatile anesthetics
- Patient-related risk factors:
- Recent URI (<2 weeks)
- Asthma, COPD, chronic bronchitis
- Environmental exposures (smoke, pet dander, pollution)
- Allergic reactions (latex, medications)
- Management focuses on rapid recognition, oxygen delivery, and bronchodilator therapy (beta-2 agonists by inhalation or IV).
What To Do
Recognition
- Recognition and troubleshooting are the first priorities.
- Signs vary by phase of anesthesia:
- Intubated patient:
- Difficulty ventilating
- Increased peak inspiratory pressures
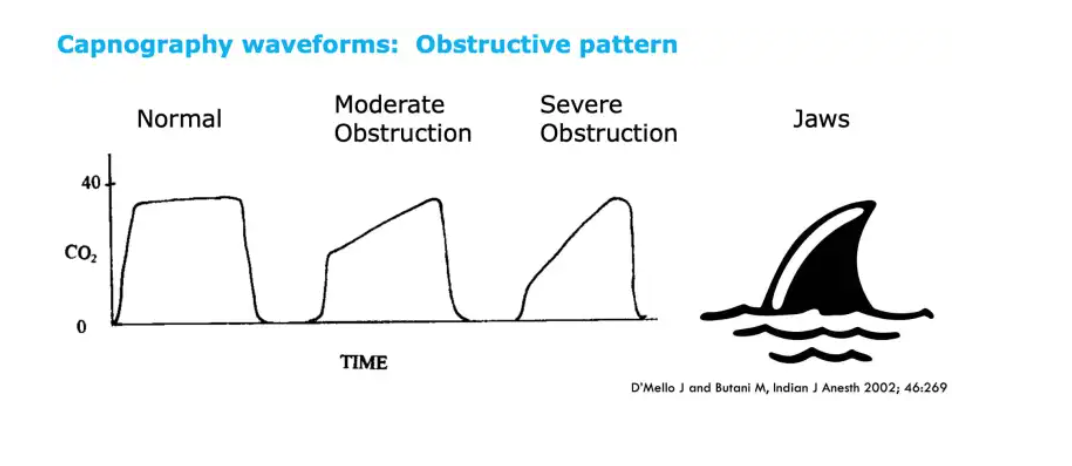
- “Shark-fin” capnography waveform
- Low or absent ETCO₂
- Decreased/absent breath sounds or wheezing
- Coughing
- Hypoxia, hypercapnia
- Intubated patient:
Management
Intubated Patient
- Increase FiO₂ to 100% and hand-ventilate.
- Deepen anesthesia (e.g., propofol bolus).
- Troubleshoot:
- Auscultate breath sounds
- Check for kinked or mainstem ETT
- Suction secretions
- Albuterol MDI via ETT (10 puffs).
- If severe: Epinephrine 10–50 mcg IV (max 1 mg).
- Additional options:
- Chest X-ray
- Ketamine or magnesium IV
- Anticholinergics: inhaled ipratropium, IV glycopyrrolate or atropine
Non-Intubated Patient
- Supplemental O₂.
- Auscultate lungs; rule out stridor.
- Albuterol nebulizer (2.5 mg).
- Administer IV steroids.
- If severe:
- Epinephrine 10–50 mcg IV (max 1 mg)
- OR 10 mcg/kg IM/SC (max 0.5 mg)
- Consider CXR, and intubation if worsening.
SCOPe Guide
Clinical Optimization
Preoperative
- Identify at-risk patients; ensure pre-op inhaler use.
- Thorough history:
- Known triggers
- Recent exacerbations or ER visits
- Oral glucocorticoid use
- Severity/frequency of asthma attacks
- Baseline PEF or FEV₁
- Premedication:
- Albuterol 2–4 puffs or nebulizer 20–30 min before induction
- Anticholinergics to reduce vagal tone & secretions
Intraoperative
- Consider regional vs general anesthesia.
- Induction choices:
- Sevoflurane → potent bronchodilator
- IV agents: lidocaine, propofol, opioids blunt reflexes
- Ketamine → bronchodilation
- Dexmedetomidine may prevent bronchoconstriction
- Maintain adequate depth of anesthesia.
- Manipulate airway only under deep anesthesia.
- Suction can be a trigger; use carefully.
- SGA may be less stimulating than ETT in select patients.
- Use selective beta blockers cautiously.
- Reversal agents:
- Sugammadex may induce bronchospasm in patients with pulmonary disease.
Emergence
- Suction airway thoroughly.
- Extubate either fully awake or deep.
- Albuterol prior to emergence if needed.
Postoperative (PACU)
- Breathing treatments PRN.
- Handoff should include:
- Medications given
- Bronchospasm events
- Relevant pulmonary history
Pearls
- Optimize at-risk patients prior to induction.
- Tailor anesthetic plan to pulmonary history.
- Recognition and rapid management are key.
- Oxygen, Albuterol, Epinephrine if severe.
- Remember: “If I can’t breathe, Look, Listen & Remember OAE is KEY!”
Quick Resources
- OpenAnesthesia: Bronchospasm
- UpToDate: Anesthesia for adult patients with asthma
- Hines RL, Marschall KE. Stoelting’s Anesthesia and Co-Existing Disease. 7th ed. Elsevier; 2018: 19–22, 65.
Media