Bougie/ETT Introducer
Kristin Barkley, DNP, CRNA
Bougie
Quick Facts
- Endotracheal tube (ETT) introducer and essential adjunct for difficult intubation.
- Often called a “gum” bougie; typically 50–70 cm, semi-rigid, with a curved distal coudé tip.
- Coudé tip facilitates anterior advancement under the epiglottis into the glottic opening.
- High first-pass success reported in emergency intubations when used appropriately.
- Use cases: primary intubation aid, extraluminal ETT exchange, adjunct with videolaryngoscopy, cricothyrotomy assistance.
Procedure Guide
Sizes
- Standard adult: ~15 Fr (typically accommodates ≥6.0 ETT).
- Pediatric and neonatal sizes available.
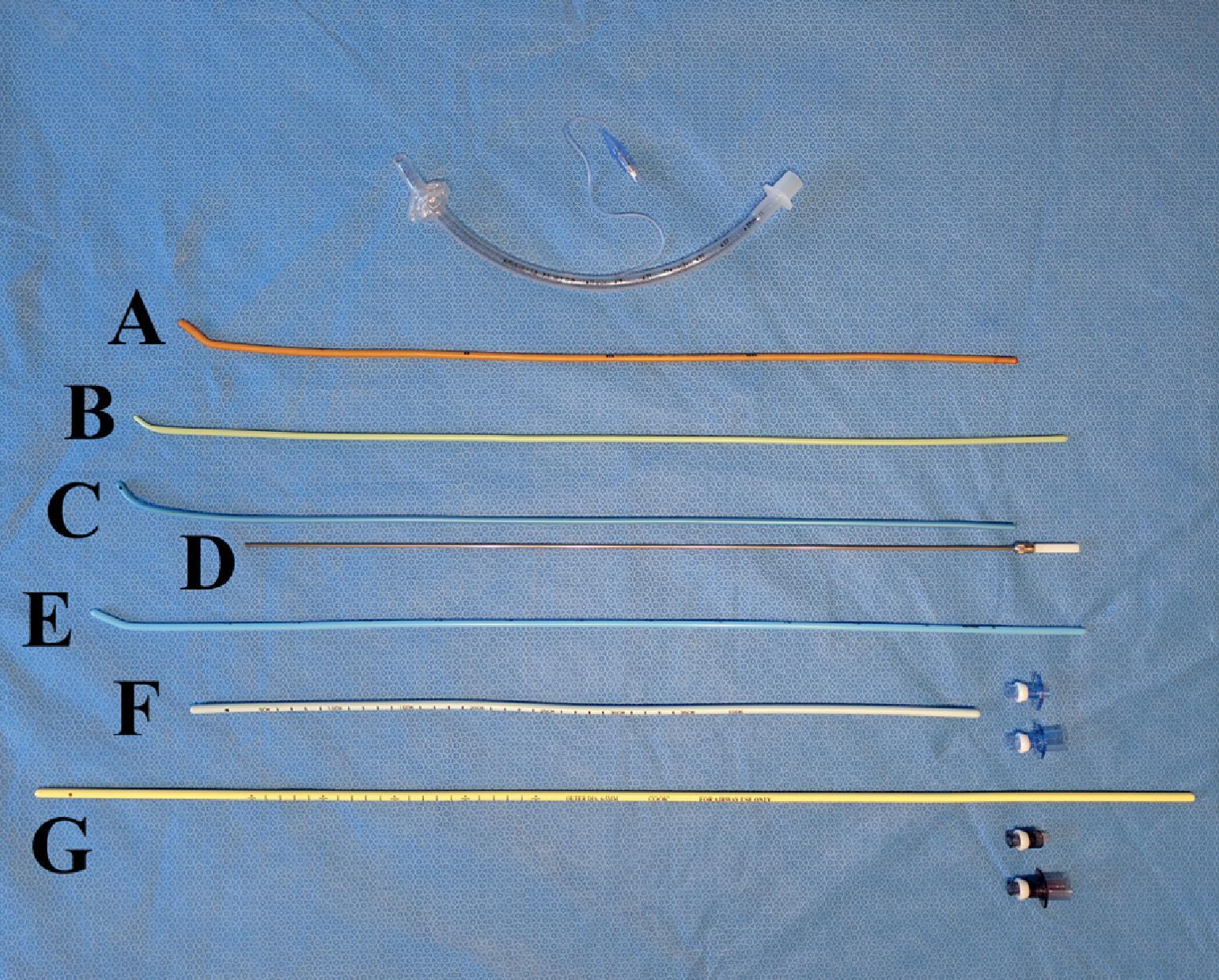
Types
- Eschmann: woven rod with resin coating; classic reusable “gum” bougie.
- Standard disposable: single-use introducers.
- Steerable: controllable anterior/posterior tip deflection for anterior laryngeal inlet.
- Frova: hollow, fenestrated tip allows oxygenation/jet ventilation options.
Indications / When to Use
- Failed or difficult intubation—especially when epiglottis seen but cords not fully visualized.
- Grade III Cormack-Lehane view (partial/absent glottic view), anterior glottis, anatomic difficulty, or obstruction.
- Usable with direct or video laryngoscopy (may be more challenging with hyperangulated blades).
Key Notes
- Apply lubricant to improve ETT railroading over the introducer.
- Standard bougie/ETT introducer has a curved coudé tip; dedicated exchange catheters differ in length/lumen and are designed for tube exchanges, double-lumen ETTs, or SGA exchanges.
- Standard bougie does not fit inside a double-lumen ETT.
Placement Technique
- Insert laryngoscope and identify epiglottis; advance bougie with the tip directed anteriorly, sweeping under the epiglottis toward trachea.
- Tactile confirmation: feel “clicks” as tip passes tracheal rings; advance ceases with gentle resistance at ~24–40 cm (small airways). Do not force.
- Railroad the ETT over the bougie into the trachea; keep laryngoscope in place to maintain tongue displacement and glottic exposure (often requires a second practitioner).
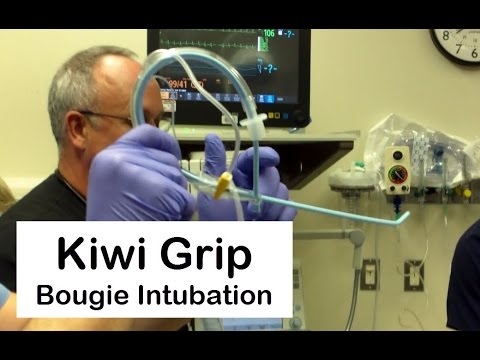
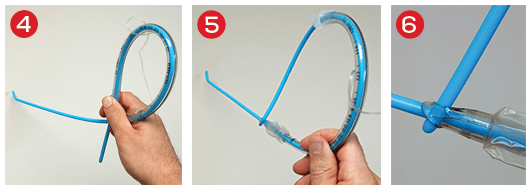
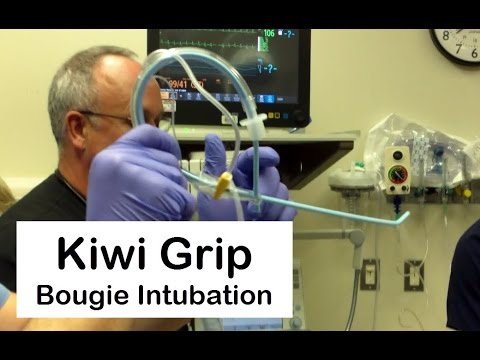
- Single-operator option: Pre-load ETT with a 90° bend (Kiwi-D grip) or through the Murphy eye to facilitate advancement.
Troubleshooting
- Size mismatch can catch at arytenoids—use a bougie size appropriate to the ETT.
- If hang-up occurs, rotate the introducer counterclockwise and re-advance gently.
- If resistance when railroading ETT, rotate tube counterclockwise and attempt again; never force.
SCOPe Guide
Strategies
- Pre-shape: Manually curve the distal 10–20 cm (≤30° bend) to improve midline entry and avoid the tongue base.
- Entry path: If uncurved, enter from right side and sweep midline with laryngoscope.
- Targeting: Identify the epiglottis; advance tip anteriorly beneath it toward the glottis.
- Railroad: Keep the laryngoscope in place while advancing the ETT over the bougie.
Clinical Optimization
- Verify bougie availability during routine OR setup (e.g., SAMMTIDE checklist).
- Maintain coudé tip orientation—avoid unintended rotation posteriorly or laterally.
- Never force the bougie or ETT when resistance is met—adjust rotation, position, or view.
Pearls
- Most ORs stock bougies in the standard airway setup—confirm correct size and ETT compatibility (standard adult bougie supports ≥6.0 ETT).
- Lubricate when possible to ease railroading.
- Master both two-person and solo (pre-loaded) techniques.
- Maintain laryngoscope position throughout; feel for tracheal “clicks” and stop at resistance.
- If the bougie advances “too far” without clicks or resistance, reassess—likely esophageal placement.
Media
- Intubating introducers and lighted/optical stylets (overview)
- Bougie demonstration (thumbnail)
- Bougie usage graphic (ACEP)
References
- UpToDate: Endotracheal tube introducers (gum elastic bougie) for emergency intubation
- Barash PG, Cullen BF, Stoelting RK, et al. Clinical Anesthesia. 8th ed. Wolters Kluwer; 2017.
Media Attributions
- 0_3s20B9780323795388000229
- 0
- feature-story_pg22c

{kind=link}
{kind=link}